 Are infectious and unrecognized
bacteria involved in the cause of prostate cancer? Can so-called "cancer
microbes" cause cancer? Is there a connection between prostate cancer
and a cancer-causing virus common in AIDS patients? These controversial
questions concerning the cause of prostate cancer are explored here. In
addition, microphotographs of the newly-discovered bacteria found in prostate
cancer are presented. Are infectious and unrecognized
bacteria involved in the cause of prostate cancer? Can so-called "cancer
microbes" cause cancer? Is there a connection between prostate cancer
and a cancer-causing virus common in AIDS patients? These controversial
questions concerning the cause of prostate cancer are explored here. In
addition, microphotographs of the newly-discovered bacteria found in prostate
cancer are presented.
-
- Prostate cancer is the most common form of cancer in
American men, with 230,000 new cases diagnosed yearly and 30,000 deaths
annually (double the number of yearly AIDS deaths in the U.S. ). This slow-growing
cancer primarily affecting older men. Elderly men with prostate cancer
often die from some other cause.
-
- Autopsy studies have shown that by the time men reach
age 50, already thirty percent of men have microscopic evidence of prostate
cancer; and at age 80 there is an 80% chance a man will have this cancer.
Standard treatment is surgical removal of the entire gland (along with
a portion of the urethra contained within it) or a series of radiation
treatments to the prostate. Both procedures often result in urinary incontinence
and impotence.
-
- Since the late 1980's the PSA (prostate specific antigen)
blood test has been widely used to screen for prostate cancer. Previously,
a rising PSA level of 4 nanograms or more signified possible cancer. However,
a new study in May 2004 indicates that 15% of men with PSA levels less
than 4 had cancer when their prostates were assessed with biopsies. The
results of this new study is causing great controversy in the diagnosis
and treatment of prostate cancer.
-
-
- What causes prostate cancer?
-
-
- Like most forms of cancer, there is no known cause. If
the cancer is confined to the prostate a cure is probable, but once it
spreads to other parts of the body, there is no cure.
- An April 2004 report widely heralded in the media suggests
that men who ejaculate more frequently might lower their risk for prostate
cancer. A May 2004 report also warned that men with a history of sexual
promiscuity and sexually-transmitted diseases were more likely to get prostate
cancer.
-
- Acute and chronic inflammation of the prostate (prostatitis)
is a common and painful condition affecting younger and middle-aged men.
The cause of chronic prostatitis is incompletely understood, although antibiotic
therapy is employed in the majority of cases. A variety of bacteria (staphylococci,
streptococci, corynebacteria, and others) have been cultured from prostatitis.
There is debate whether this ailment is a risk factor for cancer. Benign
prostatic enlargement (hyperplasia) , another common condition of older
men, is not a precursor to carcinoma.
-
- There is also disagreement regarding the role of testosterone
in the development of prostate cancer.
-
- Researchers have recently cautioned men about ingesting
excessive amounts of zinc supplements, claiming that 100 milligrams of
zinc daily could more than double the risk of prostate cancer. DHEA, another
popular supplement, is also suspect because some fear that the increased
levels of testosterone seen with daily DHEA pills could stimulate the growth
of a tiny prostate tumor that would otherwise have remained dormant.
-
-
-
- Prostate Cancer and Kaposi's sarcoma virus
infection
-
-
- Over the years a number of viruses (the cytomegalovirus,
human papilloma virus, various herpes viruses, and the hepatitis B virus)
have been suspected of causing or complicating prostate cancer. A very
recent report suggests the Kaposi's sarcoma virus, also known as human
herpes virus 8 (HHV-8), might also be involved .
-
- The Kaposi's sarcoma virus is intimately connected with
the epidemic of HIV (human immunodeficiency virus) and AIDS. Prior to the
AIDS epidemic in gay men in the late 1970's, so-called "classic"
Kaposi's sarcoma (KS) in the U.S. was a rare cancer tumor found primarily
in elderly men of Jewish and Italian extraction.
-
- When AIDS began exclusively in the gay male population
in America in the late 1970s, KS skin tumors in young homosexuals became
the "Scarlet Letter" of the new disease. Up to one-third of AIDS
patients now carry the KS virus. When AIDS began, one in three gay AIDS
patients had KS skin lesions. Now, only one in ten men with AIDS have KS
lesions.
-
- Infection with HIV makes patients more vulnerable to
certain cancers, particularly lymphoma, KS, and uterine cancer. However,
prostate cancer in HIV-infected men is uncommon.
-
- Although cases of "classic" KS were first diagnosed
in Europe in 1872, the KS virus was only discovered in 1994 in cases of
AIDS-related KS. This KS virus has also been found in other forms of cancer,
such as lymphoma and multiple myeloma.
-
- A 2004 study by LJ Hoffman and associates at the University
of Pittsburgh tested the blood of prostate cancer patients for antibodies
to the KS virus antigens. Remarkably, 40% of men from Trinidad and Tobago
and 20% of U.S. men tested positive for antibodies to the KS virus. This
was considerably higher than an age-matched control group of Trinidad men
(23%) and American men (5%). The researchers conclude that the KS virus
could play a role in the development of prostate cancer.
-
- In the U.S. the general incidence of KS virus in blood
donors is 5%. However, a 2002 study of Texas blood donors indicated a 15%
infection rate.
-
- The emergence of the KS virus worldwide indicates the
virus has been introduced in recent decades. The fact that both HIV and
the KS virus were initially introduced exclusively into the gay American
population in the late 1970s has received little comment. One can perhaps
easily explain the introduction of a new HIV virus of supposed African
origin, but what is the explanation for the additional and simultaneous
introduction of a second virus - the KS virus - into gay men?
-
- At present, the blood supply is not screened to eliminate
donors carrying the KS virus. Gay men, and any man who has had sex with
another man since 1978, are routinely banned as donors, and all blood is
screened for HIV. Yet, KS virus carriers are not excluded. This alone is
good reason for any person undergoing elective major surgery (like prostate
gland removal) to donate their own blood beforehand in the event that a
blood transfusion is needed during or after surgery.
-
-
-
- Cancer and the Cancer Microbe
-
-
- Although medical science claims the cause of most cancers
is unknown, there is evidence accumulated since the late 19th century to
show that cancer is a disease caused by infectious bacteria (not to be
confused with viruses which are not visible microscopically). In 1890 the
noted Scottish pathologist William Russell (1852-1940) discovered round
forms in cancer tissue which he interpreted as "the characteristic
organism of cancer." These forms were subsequently discredited as
infectious agents but have became known to every pathologist as "Russell
bodies." (For more details see, "The Russell Body: The forgotten
clue to the bacterial cause of cancer" at: www.rense.com/general44/russell.htm)
-
- The most vocal proponent of bacteria as a cause of cancer
was the late Virginia Livingston, M.D. In 1950, Virginia Wuerthele-Caspe
Livingston and Eleanor Alexander-Jackson (a microbiologist), along with
John A Anderson (head of the Department of Bacteriology at Rutgers), James
Hillier (head of the electron microscopy at the RCA Victor Laboratories
at Princeton), Roy Allen (a renowned microscopist), and Lawrence W Smith
(author of a well-known pathology textbook used in medical colleges), all
combined their talents to write a paper entitled "Cultural Properties
and Pathogenicity of Certain Microorganisms Obtained from Various Proliferative
and Neoplastic Diseases," published in the December issue of The American
Journal of the Medical Sciences. The characteristics of the cancer microbe
in blood, tissue, and culture, were described in detail; and the extreme
pleomorphic nature of the organism was revealed in photos taken with the
electron microscope at a magnification of 31,000X. (The ordinary light
microscope only magnifies a thousand times.)
-
- The cancer microbe, which Livingston later called Progenitor
cryptocides, was filterable through a pore designed to hold back bacteria,
indicating that the smallest forms of the microbe were indeed "virus-sized."
However, with time these filter-passing were able to grow and revert back
to the size of conventional bacteria.
-
- The microbe was characterized as pleomorphic, that is,
having more than one form and size. The smallest forms of the organism
were virus-like, and the larger bacterial forms were comparable to what
bacteriologists call "mycoplasma", "L-forms" and "cell-wall
deficient forms." The largest forms of the organism resembled what
Russell called "the cancer parasite." Livingston believed the
organism was closely related to the mycobacteria, the species of acid-fast
bacteria that causes tuberculosis. She claimed the "acid-fast"
staining method was essential to identify the microbe in tissue and in
culture.
-
- In a series of papers Livingston and her colleagues all
continued important cancer microbe research showing the characteristic
"connective tissue parasite" of cancer, the germ that could be
found inside the cell (intracellular) and outside the cell (extracellular)
in all cancers they studied. Livingston always stressed that the microbe
tends to involve the collagenous (connective) tissue, and the photographs
presented here in prostate cancer confirm that.
-
- When she died in 1990 at the age of 84, she was widely
regarded as a quack, particularly by the American Cancer Society which
claimed her cancer microbe did not exist. Likewise, a bulletin published
by the National Cancer institute on Nov 30, 1990 stated: "There is
no scientific evidence to confirm Livingston's theories of cancer causation."
-
- More details covering a century of cancer microbe research
can be found in my book, The Cancer Microbe: The Hidden Killer in Cancer,
AIDS, and Other Immune Diseases (1990) , in Cell Wall Deficient Bacteria
(1993) by Lida Mattman, Ph.D., in Can Bacteria Cause Cancer?: Alternative
Medicine Confronts Big Science (1997) by David Hess, and also by initiating
a computer search at www.google.com and typing in "cancer bacteria",
"cancer microbe", or "cancer-associated bacteria."
-
- Over the past four decades personal publications in medical
journals record the presence of cancer bacteria in various cancers, including
breast cancer, Kaposi's sarcoma, Hodgkin's disease, mycosis fungoides,
as well as in non-cancerous diseases like scleroderma, lupus erythematosus,
and sarcoidosis. Additional papers on the microbiology of cancer are presented
online at the Journal of Independent Medical Research web site (www.joimr.org).
References and abstracts on 10 cancer microbe medical publications can
be found at the National Library of Medicine's "PubMed" web site
(www.ncbi.nlm.gov/PubMed/). (Type in "Cantwell AR + cancer bacteria".
-
- According to Livingston, the cancer microbe is present
in the blood, tissue, excreta, and body fluids of all human beings. When
the immune system is functioning normally these microbes did not cause
disease. However, when tissue is damaged or weakened these microbes became
aggressive and pathogenic, producing hardening and thickening of the tissue
(such as found in scleroderma and heart disease), inflammation (autoimmune
diseases and sarcoidosis) and proliferative and cancerous changes. The
cancer microbe is essential to our life biology. When conditions are adverse,
it emerges and reverts to its pathogenic form .
-
- Livingston's research is connected with newer microbiologic
findings indicating that the blood of all human beings is infected with
a variety of so-called "cell wall deficient" bacteria. Tiny,
virus-like forms of the cancer microbes are undoubtedly related to the
tiniest of newly-discovered bacteria currently called nanobacteria. These
previously neglected and largely-unstudied nanobacteria, which lie in size
between the normal-sized bacteria and the smallest viruses, are thought
to be involved in a variety of skin and heart ailments presently labeled
as diseases of unknown etiology. An excellent source of up-to-date nanobacteria
research can be found at the Nanobac Pharmaceutical web site (www.nanobaclabs.com/research
).
-
-
-
- Detecting Acid-Fast Cancer Bacteria in Prostate
cancer
-
-
- In December 2003 my partner of 30 years was diagnosed
with prostate cancer. He is a 68 year-old Italian-American who has always
been in good health. His PSA was abnormally elevated to 9, and a digital
rectal examination by the urologist revealed a hardened area on the right
side of the gland. Multiple biopsies were performed from six areas of the
prostate gland and three were positive for adenocarcinoma.
-
- Two months before the prostate cancer diagnosis, he had
a skin biopsy performed on a small reddish skin lesion on the right lower
leg. The pathology report was interpreted as Kaposi's sarcoma. The lesion
totally disappeared after the biopsy site healed and there has been no
recurrence.
-
- In view of the frequent association of KS with AIDS,
an HIV test was performed and was negative. Thus, his KS diagnosis was
consistent with the pre-AIDS "classic" type of KS which, although
rare, is found most often in elderly Jews and Italians in America. His
blood was not tested for the KS virus. However, blood tests did reveal
past asymptomatic infection with the hepatitis B virus, and he has a history
of recurrent skin infection with herpes simplex virus.
-
- A prostatectomy, along with removal of the surrounding
lymph nodes, was performed in March 2004. Microscopic examination of this
tissue showed the cancer entirely confined to the prostate with no cancer
detected in the nodes. Approximately 25% of the gland was involved with
invasive adenocarcinoma. (Cancerous prostate glands removed at surgery
often tend to be multifocal, meaning that more than one part of the gland
is affected by cancer.)
-
- In view of my previous cancer microbe studies, I requested
that the pathologist supply me with a Fite-stained tissue section of his
prostate tissue. The Fite stain is an "acid-fast" stain traditionally
used for the detection of acid-fast tuberculosis-type bacteria. The acid-fast
stain is essential to detect cancer-associated bacteria. One of the reasons
pathologists do not identify bacteria in cancer is that the hematoxylin-
eosin tissue stain, routinely employed by pathologists for diagnosis, does
not stain cancer microbes.
-
- Because bacteria are so small, it is necessary to study
the tissue under oil immersion. That is, a drop of oil must be put on the
slide and the tissue must be studied carefully using the oil-immersion
lens of the light microscope in order to visualize the material at the
highest possible magnification. This allows tissue examination at the highest
magnification possible, a magnification of 1000 times.
-
- Having retired from dermatologic practice a decade ago,
I had done absolutely no microscopic work. Although I had studied various
types of cancer related to dermatology, I had never had the opportunity
to study prostate cancer, the leading cancer of men. I had previously reported
on bacteria in various types of KS. Learning about the association of the
KS virus and prostate cancer, I was determined to see if microbes could
be identified in my partner's cancer, particularly because he had the rarest
of cancers - the non-AIDS related classic form of KS seen in elderly Italian
men .
-
- For the first 15 minutes of study I searched the most
cancerous area of the gland and found nothing. However once I searched
the connective tissue areas (the stroma) adjacent to the main tumor mass,
the bacteria were easily detected.
-
-

- Fig 1
-
-

- Fig 2
-
-
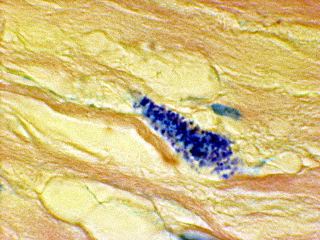
Fig 3
-
-
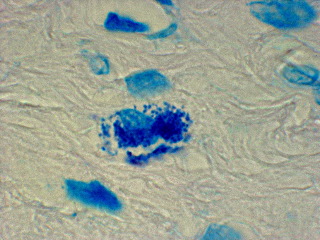
Fig 4
-
-
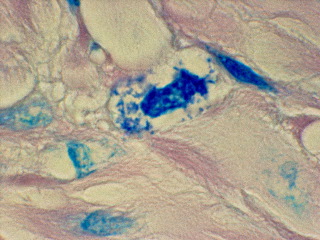
Fig 5
-
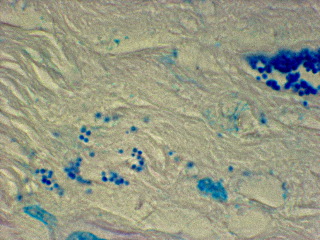
Fig 6
-
-
-
- Like bacteria observed in other forms of cancer, prostate
cancer bacteria are primarily observed in the connective tissue stroma
in tightly-packed clusters of round "coccoid" forms seemingly
embedded in a matrix. These microbes can be seen, although with difficulty,
by using the "high power" lens of the microscope, which magnifies
400 times (Figures 1 and 2). Using oil and the oil-immersion lens, which
allows magnification up to 1000 times, the organisms are seen more clearly.
The forms are primarily seen packed together in tight units in the connective
tissue stroma (Figure 3). Sometimes a cell nucleus is clearly visible in
the cluster (Figure 4). Rarely, one can see intracellular forms which suggest
short rod-shaped bacterial forms, rather than the common round coccoid
forms (Figure 5). Extracellular forms that escape from the tight bacterial
clusters can be seen scattered in the connective tissue (Figure 6). Occasionally
larger coccoid forms are seen that are three and four-times larger than
the tiniest round forms. The largest round spore-like forms seen in Figure
6 are apparently what Russell observed as his "parasite of cancer."
-
- The photos emphasize the varied size and shape of the
pleomorphic microbial forms in the prostate, as well as the preference
of the microbe for "collagen" - the "glue" protein
that helps hold together the cells and tissues of the body. Could this
affinity for collagen produce the biochemical change related to the elevated
protein antigen detected by the PSA test for cancer? Particularly when
antigens are often defined as foreign substances produced by bacteria and
viruses.
-
-
-
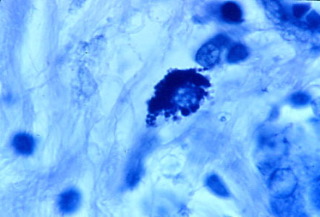
Fig 7
-
-
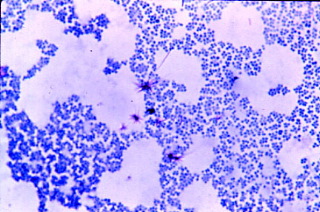
Fig 8
-
-
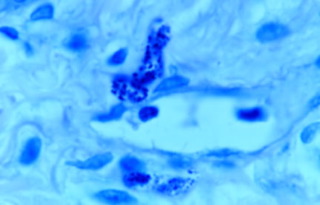
Fig 9
-
-
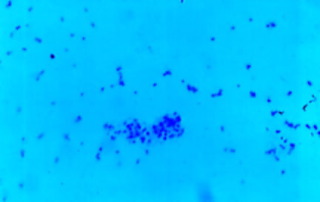
Fig 10
-
-
-
-
- Cancer Microbes and human blood
-
-
- Although doctors and blood suppliers would like the public
to believe that transfused blood is "safe" and free from harmful
infectious agents, in reality human blood is an aquarium filled with various
known and unknown viruses and bacteria. Currently, healthy blood donors
are screened for syphilis, hepatitis B and C, HIV-1 and 2, and HTLV-1 and
2. However, there is no routine screening for other known pathogenic viruses,
such as transfusion transmitted virus (TTV), hepatitis G, the KS virus,
parvo B 19 virus, and others.
- It is now increasingly recognized that everyone's blood
contains bacteria. Some of the species of blood bacteria (staphylococci,
streptococci, corynebacteria) are similar to the kinds of bacteria found
on the skin. However, these types of bacteria are also closely related,
if not identical, to what are generally and loosely termed "cancer-associated
bacteria", as reported by various investigators over the decades.
Except for the bacteria that cause syphilis, "healthy" blood
is not screened for any of these bacterial agents. Blood suppliers also
ignore a host of tiny and difficult-to-culture "nanobacteria",
which are newly-recognized normal constituents of the blood.
-
- The origin of cancer microbes in cancer tissue may very
well be derived from blood bacteria. The microbiology of cancer, although
ignored by science, will ultimately have to be explored in relationship
to the equally-ignored microbiology of human blood.
-
-
- Cancer: One disease or many?
-
- The cancer establishment believes that cancer is not
one disease but many different diseases, each with their special risk factors,
and each with their own special treatment. However, if bacteria turn out
to be the cause, cancer may prove to be essentially one disease and not
many different ones. For example, tuberculosis bacterial infection confined
to the skin is a very different clinical disease from extensive tuberculosis
infection of the lungs. Yet both diseases are the same because they are
caused by the same agent- and they are treated with the same drugs.
-
- Breast cancer and Kaposi's sarcoma are considered very
different diseases. However, cancer bacteria have been reported in both
diseases. Figures 7 shows the appearance of variably-sized intracellular
coccoid forms in breast cancer (infiltrating ductal carcinoma), and Figure
8 shows the acid-fast stained appearance of Staphylococcus epidermidis
cultured from the tumor when it metastasized to the skin. The size of some
of the coccoid forms in the tumor is exactly the size and shape of the
staphylococci bacteria cultured from the tumor. In addition, the presence
of pink and red "acid-fast spicules" sprouting from coccoid bodies
seen in the staphylococcus culture is most unusual. However, Livingston
and Alexander Jackson showed exactly the same type of acid-fast spicule
growth in culture from the urine of a cancer patient in their 1970 paper
(their Figure 12A). This research regarding "a specific type of organism
cultivated from malignancy" was presented at the New York Academy
of Sciences in November 1969. These two women repeatedly claimed the cancer
microbe was related to the acid-fast mycobacteria that cause tuberculosis
- and that the acid-fast stain was the key to identifying this microbe.
-
- Figure 9 shows coccoid forms within a skin lesion of
KS in a patient near death from AIDS. Figure 10 shows the appearance of
Streptococcus G cultured from his blood shortly before death. If one compares
the size and shape of the blood streptococci, they appear similar in size
and shape to the coccoid forms seen deep in the skin of a KS tumor .
-
- Until the recent study associating the KS virus with
prostate cancer, there was no relationship between KS and prostate cancer.
Likewise, mammary gland breast cancer and prostate cancer (found exclusively
in men) seemingly have nothing in common except they are the most common
forms of cancer (other than skin cancer) in women and men. Both the mammary
and the prostate glands are secretory glands that excrete externally, and
both glands and both cancers are hormone-fueled. But the pleomorphic coccoid
forms seen in both cancers are similar in appearance, suggesting that bacteria
are involved in the production of both these "different" cancers.
-
- If one studies the microbiology of cancer, it is apparent
that cancer microbes provoke not only cancer, but also a variety of tissue
responses, including fibrosis and thickening of the connective tissue (as
in scleroderma), cellular infiltrations (as seen in autoimmune diseases),
and the formation of tumors. The fact that similar-appearing bacteria can
be identified in acid-fast stained tissue sections of so many different
types of diseases makes them admittedly an unprecedented type of infectious
agent.
-
-
-
- Why does the medical establishment ignore
cancer microbe research?
-
-
- Despite a century of credible cancer microbe research,
the medical profession generally ignores all aspects of research implicating
bacteria in cancer. One exception is the 1982 discovery of certain bacteria
in the stomach (Helicobacter pylori) that are now accepted as the cause
of stomach ulcers that can sometimes progress to cancer and gastric lymphoma.
-
- The most influential physician condemning cancer-associated
bacteria was James Ewing, a noted American pathologist and author of the
widely read textbook, Neoplastic Diseases (1919), in which he wrote that
"few competent observers consider it (the parasitic theory) as a possible
explanation in cancer." In Ewing's view, cancer did not act like an
infection. Therefore, he reasoned microbes could not possibly cause cancer.
As a result of his edict, few doctors dared to contradict Ewing by continuing
cancer microbe research.
-
- Ewing co-founded the American Cancer Society in 1913
and in the 1930's he was the director of Memorial Hospital, now better
known as Memorial Sloan-Kettering Cancer Center in New York City, one of
the most prestigious cancer hospitals in the world. Ewing died in 1943
from bladder cancer, at the age of 76.
-
- Although bacteria were dismissed as causative agents
one hundred years ago, viruses are now considered as likely causes of cancer
- despite Ewing's contention that cancer did not act like an infectious
disease. What the pathologist did not know is that pleomorphic cancer microbes
have characteristics of both bacteria and viruses and were not visible
with routine staining methods . Although physicians now easily accept the
idea of microscopically invisible viruses in cancer, they seem unable to
conceive of a microscopically visible bacterial agent in cancer.
-
- Undoubtedly, the acceptance of cancer bacteria would
put cancer research and treatment into a tailspin cancer chemotherapy and
radiation would have to be reevaluated as a rational treatment for bacterial
infection. Because current antibiotics cannot rid the body of cancer-causing
bacteria, this would necessitate the development of new cancer treatments
designed to minimize this infection.
-
- It may be left to future medical historians to explain
why cancer microbe research has been ignored for so many years, despite
the millions of cancer deaths yearly and the billions spent on cancer research.
-
- In the meantime, as a retired physician I will continue
to bug (pun intended) my colleagues in medicine to search for acid-fast
bacteria as I and other cancer microbe researchers in the past have done.
The only requirements are an acid-fast stained histopathologic slide of
the malignant tissue, a drop of oil, the use of the oil-immersion lens,
a little patience, and an open mind.
-
- To ignore cancer bacteria because a powerful pathologist
once told his students a century ago that there were no microbes to be
found in cancer is simply irrational and bad science. Re-search means to
search again. After many decades of failure to uncover a cause for cancer,
surely it is time for a second look at bacteria that can be easily found
in this dread disease.
-
-
- Legend for Photographs
-
- Figure 1: Tissue section from prostate adenocarcinoma
showing, in center, a cluster of tightly-packed intracellular blue-stained
coccoid forms. Fite (acid-fast) stain, magnification x 400 ("high
power").
-
- Figure 2: Prostate cancer. In center, additional focus
of intracellular blue-stained coccoid forms. Fite stain, magnification
x 400 ("high power").
-
-
- Figure 3. Prostate cancer. Tightly-packed cluster of
blue and pink-stained coccoid forms in the connective tissue stroma. Fite
stain, magnification x 1000 (highest magnification), in oil.
- Figure 4. Prostate cancer. Loosely-packed intracellular
blue-stained coccoid forms. Fite stain, magnification x1000, in oil.
-
- Figure 5. Prostate cancer. Rare cluster of loosely-packed
intracellular and extracellular coccoid and tiny rod-shaped forms. Fite
stain, magnification x1000, in oil.
-
- Figure 6. Prostate cancer. On right, a cluster of larger
coccoid forms. On left, scattered larger extracellular coccoid forms in
the connective tissue stroma.
- These forms could be compatible with "Russell bodies"
- which Russell believed were "the characteristic organism of cancer."
Fite stain, magnification x1000, in oil.
-
- Figure 7. Breast cancer. In center, intracellular, tightly-packed
variably-sized coccoid forms. Kinyoun's (acid-fast) stain. magnification
x 1000, in oil.
-
- Figure 8. Smear from culture of Staphylococcus epidermidis
isolated from skin metastasis of original breast cancer shown in Figure
7. In addition to myriads of staphylococci, there are 5 areas of deep blue-stained
granules from which emanate acid-fast pink and red spicules. According
to Livingston, this is a characteristic of bacteria isolated from cancer.
Note the similar size and shape of the cocci to the coccoid forms seen
in the original tumor in Fugure 7. Ziehl-Nielson (acid-fast) stain, magnification
x 1000, in oil.
-
- Figure 9. AIDS-related Kaposi's sarcoma of the skin.
Several clusters of blue-stained coccoid forms in the deep dermis of the
skin. Fite stain, magnification x 1000, in oil.
-
- Figure 10. Streptococcus G isolated from the blood of
a fatal case of AIDS and AIDS-related Kaposi's sarcoma. The size and shape
of the streptococci are similar in size and shape to the coccoid forms
seen in the KS lesion shortly before death. Ziehl-Nielson (acid-fast) stain,
magnification x1000, in oil.
-
-
- References:
-
- Alexander-Jackson E. A specific type of microorganism
isolated from animal and human cancer: bacteriology of the organism. Growth.
1954 Mar;18(1):37-51.
-
- Baillargeon J, Deng JH, Hettler E, Harrison C, Grady
JJ, Korte LG, Alexander J, Montalvo E, Jenson HB, Gao SJ. Seroprevalence
of Kaposi's sarcoma-associated herpesvirus infection among blood donors
from Texas. Ann Epidemiol. 2001 Oct;11(7):512-8.
-
- Cantwell AR, Craggs E, Wilson JW, Swatek F. Acid-fast
bacteria as a possible cause of scleroderma. Dermatologica. 1968: 136:141-150.
-
- Cantwell AR Jr, Kelso DW. Microbial findings in cancers
of the breast and in their metastases to the skin. Implications for etiology.
J Dermatol Surg Oncol. 1981 Jun;7(6):483-91.
-
- Cantwell AR Jr, Kelso DW. Microbial findings in cancers
of the breast and in their metastases to the skin. Implications for etiology.
J Dermatol Surg Oncol. 1981 Jun;7(6):483-91.
-
- Cantwell AR, Kelso DW, Jones JE. Histologic observations
of coccoid forms suggestive of cell wall deficient bacteria in cutaneous
and systemic lupus erythematosus. Int J Dermatol. 1982 Nov;21(9):526-37.
-
- Cantwell AR Jr, Kelso DW. Variably acid-fast bacteria
in a fatal case of Hodgkin's disease. Arch Dermatol. 1984 Mar;120(3):401-2.
-
- Cantwell AR. Histologic observations of variably acid-fast
pleomorphic bacteria in systemic sarcoidosis: a report of 3 cases. Growth.
1982 Summer;46(2):113-25.
-
- Cantwell AR. Variably acid-fast cell wall-deficient bacteria
as a possible cause of dermatologic disease. In, Domingue GJ (Ed). Cell
Wall Deficient Bacteria. Reading: Addison-Wesley Publishing Co; 1982. Pp.
321-360.
-
- Cantwell AR, Rowe L. African "eosinophilic bodies"
in vivo in two American men with Kaposi's sarcoma and AIDS. J Dermatol
Surg Oncol. 1985 Apr;11(4):408-12.
-
- Cantwell A. The Cancer Microbe. Los Angeles: Aries Rising
Press; 1990.
-
- Diller IC, Diller WF. Intracellular acid-fast organisms
isolated from malignant tissues. Trans Amer Micr Soc. 1965; 84:138-148.
-
- Ewing J. The parasitic theory. In, Ewing J (Ed), Neoplastic
Diseases (Ed 1); Philadelphia: Saunders; 1919. Pp 114-126.
-
- Gaylord HR. The protozoon of cancer. Amer J Med Sci.
1901;121:501-539.
-
- Glover TJ. The bacteriology of cancer. Canada Lancet
Pract. 1930; 75:92-111.
-
- Hess D. Can Bacteria Cause Cancer? New York:New York
University Press; 1997.
-
- Hoffman LJ, Bunker CH, Pellett PE, Trump DL, Patrick
AL, Dollard SC, Keenan HA, Jenkins FJ. Elevated seroprevalence of human
herpesvirus 8 among men with prostate cancer. J Infect Dis. 2004 Jan 1;189(1):15-20.
- Mattman LH. Cell Wall Deficient Forms (Ed 2). Boca Raton:CRC
Press; 1993.
-
|