- http://www.zimp.org/stuff/03%20-%20WalkerDepositionDepo.htm
-
- Court Document
-
- November 21, 2003, deposition
- (excerpts) taken from Dr. Walker, a board-certified radiologist
at Manatee Memorial Hospital. Dr. Walker is the doctor that prepared the
bone-scan report from the image of Terri Schiavo taken on March 5, 1991.
-
- 15 Q What is a total-body bone scan used
for
- 16 typically?
- 17 A It's to look for abnormalities of the
- 18 bone, whether they -- if they would be recent
- 19 abnormalities.
- 20 Q Recent --
- 21 A Recent.
- 22 Q -- abnormalities?
- 23 A Correct.
- 24 Q Is it also a technique to diagnose
- 25 osteoporosis?
-
- 1 A No.
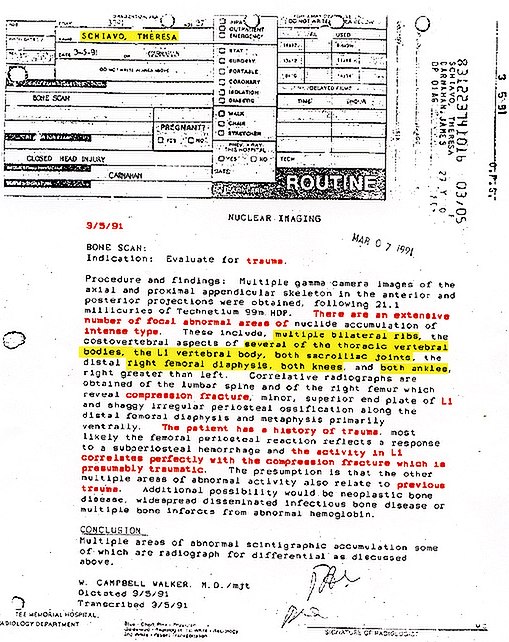
- 3 Q And the next sentence, "There are
an
- 4 extensive number of focal abnormal areas of nuclide
- 5 accumulation of intense type." What does
that mean?
- 6 A Well, that means that there are a lot
of
- 7 areas that look black on the images because lots
of
- 8 that radioactive decaying material was happening
at
- 9 those points and was being recorded by the imaging
- 10 system.
- 11 Q Okay. "These include multiple
bilateral
- 12 ribs." What would that mean to you?
- 13 A Well, you know, there's left ribs and
- 14 right ribs. And that would mean that more than
two
- 15 ribs on each side were involved.
- 13 Q "Several of the thoracic vertebral
- 14 bodies, the L1 vertebral body, both sacroiliac
- 15 joints." These are all areas that were abnormal
on
- 16 the scan?
- 17 A That's what this indicates, yes.
- 18 Q "The distal right femoral diaphysis,"
- 19 what area of the body is that?
- 20 A That would be the right leg, the upper
- 21 part of the right leg.
- 22 Q Distal?
- 23 A Above the knee.
-
- 5 Q So on the thigh bone above the kneecap
- 6 but not involving the joint?
- 7 A That's what that particular thing says,
- 8 but I think somewhere in there also, it mentioned
- 9 that both knees --
- 10 Q Right. Right after that.
- 11 A Right after that. So that's different
- 12 from the knee activity.
- 13 Q And, "Both ankles, right greater
than
- 14 left." Those are two additional areas that
showed
- 15 up as abnormalities on the scan?
- 16 A That's correct. Correct.
- 13 Q Would you draw any conclusions from
that
- 14 how old the ossification was?
- 15 A You could say that it wasn't real old,
- 16 because typically, as we mentioned, the bone is
a
- 17 dynamic structure, and it's constantly being
- 18 remodeled normally. So the body tends to take
away
- 19 extra bone eventually to remodel it to look like
- 20 normal bone. So typically old bone injuries are
- 21 remodeled so that eventually they may almost
- 22 disappear, particularly in young people. In the
- 23 very young, a fracture you won't even see in three
- 24 or four years, it will be totally erased.
-
-
- 8 Q Then you go on to say, "Most likely
the
- 9 femoral periosteal reaction reflects a response
to a
- 10 subperiosteal hemorrhage." Would that be
a bone
- 11 bruise?
- 12 A Correct.
- 16 Q Then you go on to say, "And the
activity
- 17 in L1 correlates perfectly with the compression
- 18 fracture which is presumably traumatic."
- 19 A That's what it says.
- 20 Q In other words, the x-ray confirmed
the
- 21 L1 fracture?
- 22 A The x-ray shows an abnormality at L1
- 23 which happens to correspond with the abnormal bone
- 24 turnover on the bone scan at that point.
-
- 7 Q Is this compression fracture, then,
in
- 8 common parlance, a broken back?
- 9 A Yes.
- 10 Q Is there any way to tell how old that
- 11 fracture would be?
- 12 A Well, as I've alluded to, the bone scan
- 13 gives some suggestion of that.
- 14 Q More recent rather than less recent?
- 15 A Correct. Typically in trauma the rule
of
- 16 thumb is that a traumatic fracture is not active
on
- 17 the bone scan after 12 to 18 months.
-
-
- 9 Q The report goes on to say, "The
- 10 presumption is that the other multiple areas of
- 11 abnormal activity also relate to previous trauma."
- 12 A That's what it says.
- 13 Q And, again, that's based on the fact
that
- 14 Dr. Carnahan is a rehab physician, that you were
- 15 asked to evaluate for trauma?
- 16 A And the pattern of activity is fairly
- 17 typical of multiple traumatic injuries of relatively
- 18 recent origin.
- 19 Q I realize you can't assign a cause to
- 20 these injuries that you picked up in this report.
- 21 But typically in your experience, what would be
the
- 22 causes of this pattern of abnormality?
- 23 A In somebody her age, an auto accident
is
- 24 by far the most typical cause.
- 25 Q Assume that she was not in an auto
-
- 1 accident but that she had suffered an anoxic or
- 2 hypoxic encephalopathy type of injury from a cardiac
- 3 arrest and had been bedridden for a year at this
- 4 point. What might account for these abnormalities?
- 5 A In my knowledge, that type of injury
- 6 would not account for this pattern of abnormalities.
-
- 5 Q Okay. Is this a pattern of heterotrophic
- 6 ossification as reported in the literature that
you
- 7 looked at?
- 8 A Not typically.
- 9 Q What makes it atypical?
- 10 A Well, if I were to pick one thing, I
- 11 would say the activity in the ribs is not typical.
- 12 And typically heterotrophic ossification occurs
- 13 around the joints because they're not being moved.
- 14 And typically you will see on the radiographs
- 15 calcium deposits actually sitting there. And they
- 16 don't look like periosteal reaction typically
- 17 either; they have a different appearance.
-
- 4 Q Can you say, then, within a reasonable
- 5 degree of medical certainty whether this bone scan
- 6 is consistent with heterotrophic ossification?
- 7 A In my knowledge, it's not consistent
with
- 8 heterotrophic ossification as I typically see it.
-
- 21 Q Okay. And later on in your direct
- 22 examination you were saying that traumatic fractures
- 23 typically are not active on a bone scan after 12
to
- 24 18 months. Is that correct?
- 25 A That's correct.
- 19 Q Okay. Is there any way for you to say
- 20 from looking at this report when any of these
- 21 occurrences took place that caused the abnormality
- 22 to appear on the bone scan?
- 23 A I can only say that if they were
- 24 traumatic that they probably occurred within 18
- 25 months.
-
- 1 Q Is it possible that the abnormalities
- 2 that you noted on the right femoral diaphysis and
- 3 metaphysis could have occurred if the patient was
- 4 standing and suffered a cardiac arrest and fell
to
- 5 the floor?
- 6 A Probably not. That wouldn't be a typical
- 7 mechanism of injury that would cause a periosteal
- 8 bruise. Typically you need a direct blow of some
- 9 kind. I suppose one could speculate that she fell
- 10 on a piece of furniture, that that could produce
- 11 that injury. But just typically falling on the
- 12 floor would not do that.
-
- 9 Q Okay. The bone scan and radiographic
- 10 report shows only one fracture. And that is a
- 11 compression fracture to L1. Correct?
- 12 A Well, I should clarify that by stating
- 13 that not all of the areas of bone-scan abnormality
- 14 were imaged concurrently. Okay. And that's
- 15 important. In other words, we didn't x-ray every
- 16 area that was hot on there. A couple of typical
- 17 areas were imaged but not all. Of those areas
that
- 18 were imaged, the only area that showed what was
a
- 19 clear fracture was L1.
-
- 2 Q The radiographs did not show any
- 3 fractures of the right femur. Correct?
- 4 A They don't show a typical fracture.
They
- 5 show periosteal reaction, which could be the result
- 6 of a bone bruise, which is a bone injury that's
not
- 7 a loss of continuity of the structure of the bone.
- 8 So to the extent that you define fracture as a
loss
- 9 of structural continuity, then, yes, that is an
- 10 actual fracture as is typically described.
- 10 Q Okay. If an immobile patient is going
- 11 through physical therapy and part of the physical
- 12 therapy is to have manual manipulation of the legs,
- 13 particularly flexing of the knees, is it possible
- 14 that that physical therapy would result in an
- 15 abnormal appearance on a bone scan?
- 16 MS. ANDERSON: Objection. That question,
- 17 I think, is virtually unanswerable because
it
- 18 is so vague.
- 19 A I could only speculate.
- 20 Q Okay. In your opinion, is that something
- 21 that would show up on a bone scan?
- 22 A I would think only if the joint were
- 23 injured would it show up on a bone scan. Just
- 24 simple manipulation of an injured part should not
- 25 show up as an abnormality on a bone scan.
- 22 Q Would a kick be the kind of direct blow
- 23 that would produce that femoral abnormality?
- 24 A That would be a possibility, yes.
- 25 Q Would being thrown into a sharp furniture
-
- 1 corner?
- 2 A That would be a possibility.
- 3 Q Would being struck with some sort of
- 4 blunt object like a golf club or something do it?
- 5 A Yes.
- 22 Q You mentioned that you have seen
- 23 fractures in bedridden patients before?
- 24 A Yes.
- 25 Q How frequently have you seen that?
-
- 1 A Rare.
- 2 Q It's rare?
- 3 A Yes.
-
|