- Why does the medical establishment ignore a century of
research pointing to tuberculosis-type "acid-fast" bacteria
as the cause of cancer? TB-type bacteria can be seen in specially-stained
tissue sections of cancer tumors and viewed under the highest magnification
of the light microscope at a magnification of 1000 times, under oil immersion.
So why isn't this simple microscopic procedure performed in cancer?
-
- As long ago as 1890, Scottish pathologist William Russell
discovered "a characteristic organism of cancer" in every
cancer he examined; and other pathologists of that era confirmed his
findings. Yet, a century ago, the powers-that-be in medical science ignored
this research and declared emphatically that bacteria were not the cause
of cancer. The reasoning behind this dictum was that cancer did not
act like an infectious disease, nor was it communicable. We know now
this reasoning was false. Many scientists believe viruses cause cancer;
and sexually- transmitted cancer-causing viruses can be passed from person-to-
person as well.
-
- For more than a half-century, the cancer microbe has
been reported as a pleomorphic, intermittently acid-fast bacterium closely
related to the acid-fast mycobacteria and to Mycobacterium tuberculosis,
the acid-fast microbe that causes tuberculosis (TB). The acid-fast stain
is a time-honored laboratory stain specifically used to detect TB-type
mycobacteria in tissue and in culture. Virginia Livingston M.D. (1906-1990)
was the foremost proponent of the bacterial cause of cancer. She was the
first to discover that the acid-fast stain was the key to the detection
of the cancer germ, both in tissue (in vivo) and in laboratory culture
(in vitro). Livingston, along with microbiologist Eleanor Alexander- Jackson,
cell cytologist Irene Diller, and chemist and TB expert Florence Seibert,
all reported that the cancer germ was pleomorphic (meaning it has various
appearing growth forms) and was filterable, indicating that in certain
stages of its life cycle the microbe was virus-like and submicroscopic.
Bacteria can be seen with the light microscope; the much smaller viruses
cannot. (For more information on the acid-fast stain, mycobacteria, and
pleomorphism, simply Google those key words.)
-
- What do the bacteria in cancer look like? Cancer microbes
in vivo are primarily in the cell-wall-deficient (CWD) form. As a result
of the loss of a cell wall, the bacteria appear as round, coccus-like,
granular forms that are found both within the cell (intracellular) and
outside the cell (extracellular). Various types of bacteria may all look
similar when in the CWD form. In the body and in the laboratory CWD bacteria
(also known as "mycoplasma") have the amazing capacity to enlarge
in size. These so-called round "large bodies" can attain the
size of red blood cells and even larger. When seen in cancerous tissue
these large bodies of bacteria can resemble large spore forms of yeasts
and fungi, perhaps explaining why some researchers claim Candida and other
fungi are the cause of cancer.
-
- Russell's nineteenth century "parasite of cancer"
is now recognized by pathologists as "Russell bodies." Pathologists
generally believe these large forms are "immunoglobulins" and
they do not accept them as microbial in origin. It is my contention that
Russell bodies represent large, variably-sized CWD forms of bacteria
in vivo; and that is why both coccal forms of CWD bacteria, as well as
Russell bodies, can both be identified in cancerous tissue. (For more
details and microphotographs, see my paper "The Russell body: The
forgotten clue to the bacterial cause of cancer," posted on the joimr.org
and the rense.com websites; and view my video lecture "The cancer
microbe and the Russell body," currently available on Youtube.com.)
-
- Why aren't cancer bacteria recognized by pathologists
and oncologists? As mentioned, bacteria were excluded a century
ago, and medical science never looked back. The result was that any physician
who persisted in cancer microbe research was never taken seriously and
was often viewed as a medical pariah. There are less than a handful of
living physicians in the world who actively promote cancer microbe research.
Erik Enby is a 70 year-old Swedish physician, whose accomplishments are
cited in the Wikipedia. Nevertheless, his medical license has recently
been revoked by the government for his belief in cancer-causing bacteria.
I am currently regarded by the Wikipedia as a "conspiracy theorist
in the field of cancer microbiology."
-
- Although largely ignored, the microbiology of cancer
has a rich history. Details of this research can be found in my books,
The Cancer Microbe, and Four Women Against Cancer: Bacteria, Cancer,
and the Origin of Life.
-
- At present, doctors generally regard cancer-associated
bacteria as laboratory "contaminants" of no consequence, or
as "secondary invaders" of diseased tissue. However, cancer
bacteria can be observed in precancerous conditions and in areas distant
from the tumor. In general, microbiologists have been silent regarding
bacteria in cancer and some remain skeptical about bacterial pleomorphism.
Over the past decade British microbiologist Milton Wainwright has written
extensively about the history of the cancer microbe and his reports are
easily accessible on the Net. In Current Trends in Microbiology in 2006,
he wrote: "There are signs that more consideration is being given
towards the potential role of non-virus microorganisms in cancer, a fact
reflected in the recent appearance of major reviews on the subject, and
the consideration of novel approaches such as the possible role of nanobacteria
in carcinogenesis. It remains probable however, that until the potential
role of non-virus microorganisms in carcinogenesis is taken seriously,
and a massive research effort is directed towards determining their role
in carcinogenesis, we will face another century when the solution to the
enigma of cancer may be staring us in the face, only to remain ignored."
-
- In retrospect, it was premature and irrational a century
ago to discard bacteria in cancer because the science of bacteriology
was in its infancy. Nothing was known about CWD forms and filterable
virus-like forms of bacteria. The recent acceptance (after a century)
of bacteria (Helicobacter pylori) as the cause of most stomach ulcers
is a case in point. For several decades after his 1940 discovery of peculiar
S-shaped bacteria in stomach ulcers, A. Stone Freedberg MD stood alone.
His research was totally ignored because doctors believed that bacteria
could not exist in the acid environment of the stomach. A half century
later, these same bacteria were finally accepted and are now a major
factor in the development of stomach cancer. Two Australian scientists
(Barry Marshall and Robin Warren) received a Nobel Prize in Medicine in
2005 for proving this. Interestingly, in 1998, a new tumor-like stomach
lesion was discovered called "Russell body gastritis."
-
- In order to recognize CWD bacteria in cancer in vivo,
one must know what they look like. Physicians are taught that bacteria
have a certain fixed type of appearance. Most know little about the
pleomorphism of CWD bacteria, particularly the acid-fast mycobacteria.
In TB the microscopic appearance of the typical red- staining "acid-fast"
rod-shaped bacillus of M. tuberculosis is well-known. However, the pleomorphic
CWD forms of M. tuberculosis and mycobacteria look entirely different
from the typical rod form. CWD forms in vivo appear primarily as small,
round coccal and granular forms. They stain poorly, if at all, with
the time-honored Gram stain for bacteria. In addition, the routine stain
(hematoxylin-eosin stain) used by pathologists to diagnose cancer is
not suitable to demonstrate CWD bacteria. To demonstrate the typical red-staining
rods of M. tuberculosis, an "acid-fast" stain in required.
-
- Likewise, in cancer an acid-fast stain is necessary.
However, in cancer it is almost impossible to find acid-fast rods typical
of mycobacteria. As a result of all this, CWD bacteria in cancer are
not recognized; and the large body forms are passed over as Russell bodies
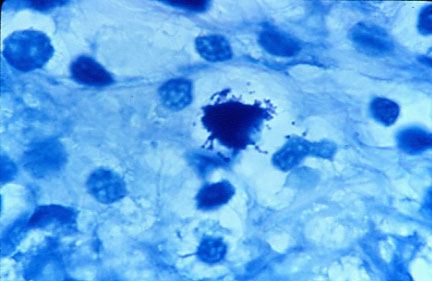
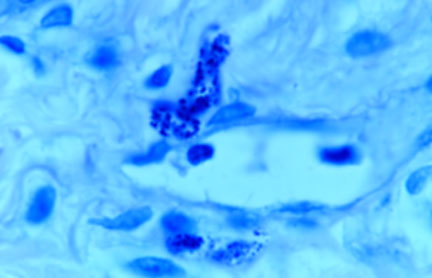
of dubious significance. Examples of the microscopic appearance of intra-
and extracellular cancer microbes in acid-fast stained tissue sections
(viewed at a magnification of 1000 times, in oil) are shown in breast
cancer, lung cancer, Hodgkin's disease (lymphoma), Kaposi's sarcoma, AIDS-related
immunoblastic sarcoma, and prostate cancer in Figures 1-7. Note that
the microscopic appearance of CWD bacteria in vivo appears similar
in various types of cancer, and consists primarily of small coccoid forms,
resembling the size and shape of ordinary staphylococci.
-
-
- Fig 1
-
-
- Fig 2
-
-
- Fig 3
-
-
- Fig 4
-
-
-
- Fig 5
-
-
-
- Fig 6
-
-
- Fig 7
-
-
-
- Can the cancer microbe be seen in diseases other than
cancer? Further complicating the bacteriology of cancer is the observation
that similar-appearing microbes can be seen in vivo in certain chronic
diseases, such as lupus, scleroderma, sarcoidosis, and others.(For details,
consult my papers posted on the joimr.org website.) Livingston claimed
that all human beings carried cancer microbes; and she postulated these
microbes were closely connected with the origin of life. In the healthy
state these microbes caused no harm and were beneficial. However, when
the immune system was weakened, these bacteria were capable of inducing
a variety of human illnesses, including cancer. CWD bacteria may
- prove to be the cause of many illnesses currently regarded
as "of unknown etiology." Because submicroscopic forms of CWD
bacteria are virus-sized, they may be confused with ordinary viruses.
CWD bacteria are also resistant to antibiotics and are difficult (if
not impossible) to eradicate or subdue, at least in the current state
of our knowledge.
-
- Are these microbes the true cause of cancer? Although
bacteria can be identified in cancer, there are obviously other well-known
factors that can induce cancer, such as sunlight in skin cancer, smoking
in lung cancer, radiation-induced cancer, etc. But in each case it may
require these ever-present bacteria to induce the cellular changes of
cancer. The demonstration that these microbes are found within the cell
and even within the nucleus (as shown by Irene Diller) indicates that
these agents may access the genetic material of the cell, thereby transforming
the cell to a cancerous state. In this respect, CWD forms may act like
viruses. Studies by Douglas Robinson MD show that bacteria (like viruses)
may swap genes back and forth between the infected cell and the microbe.
-
- If cancer is finally accepted as an infection with bacteria
it could explain why some people develop two or more different kinds
of cancer in their lifetime. At present, physicians believe each type
of cancer is different, each requiring its own special type of treatment.
Because physicians do not believe in the existence of a cancer microbe,
there has been no therapy devised to treat this infection. In my view,
Virginia Livingston's greatest contribution was her observation that the
microbe could be detected in all cancers in vivo with an acid-fast stain.
Only when physicians learn to recognize and accept these infectious bacteria
in cancer can we begin to design appropriate therapies against them.
-
- (Dr. Cantwell is a retired dermatologist. A full list
of his published scientific reports can be found at the PubMed website.
-
- His books are available through Aries Rising Press (www.ariesrisingpress.com)
and also through Amazon.com and Book Clearing House @ 1-800-431-1579.
E-mail: alancantwell@sbcglobal.net.)
-
-
-
-
- Selected Bibliography:
-
- Alexander-Jackson E. A specific type of microorganism
isolated from animal and human cancer: bacteriology of the organism. Growth.
1954 Mar;18(1):37-51.
-
- Broxmeyer L.Is cancer just an incurable infectious disease?
Med Hypotheses. 2004;63(6):986-96. Review.
-
- Cantwell AR, Craggs E, Wilson JW, Swatek F. Acid-fast
bacteria as a possible cause of scleroderma. Dermatologica. 1968: 136:141-150.
-
- Cantwell AR. Histologic forms resembling "large
bodies" in scleroderma and pseudoscleroderma. Amer J Dermatopathol.
1980; 2:273-276.
-
- Cantwell AR, Rowe L. African "eosinophilic bodies"
in vivo in two American men with Kaposi's sarcoma and AIDS. J Dermatol
Surg Oncol. 1985 Apr;11(4):408-12.
-
- Cantwell AR, Kelso DW, Jones JE. Histologic observations
of coccoid forms suggestive of cell wall deficient bacteria in cutaneous
and systemic lupus erythematosus.
- Int J Dermatol. 1982 Nov;21(9):526-37.
-
- Cantwell AR. Variably acid-fast cell wall-deficient bacteria
as a possible cause of dermatologic disease. In, Domingue GJ (Ed). Cell
Wall Deficient Bacteria. Reading: Addison-Wesley Publishing Co; 1982.
Pp. 321-360.
-
- Cantwell A. The Cancer Microbe. Los Angeles: Aries Rising
Press; 1990.
-
- Cantwell A. Four Women Against Cancer: Bacteria, Cancer
and the Origin of Life, Los Angeles: Aries Rising Press; 2005.
-
- Dienes L. Morphology and reproductive processes of bacteria
with defective cell walls. In, Guze LB (Ed). Microbial Protoplasts,
Spheroplasts and L-Forms. Baltimore: Williams & Wilkins Company; 1968,
Pp 74-93.
-
- Diller IC, Diller WF. Intracellular acid-fast organisms
isolated from malignant tissues. Trans Amer Micr Soc. 1965; 84:138-148.
-
- Ewing J. The parasitic theory. In, Ewing J (Ed), Neoplastic
Diseases (Ed 1); Philadelphia: Saunders; 1919. Pp 114-126.
-
- Gaylord HR. The protozoon of cancer. Amer J Med Sci.
1901;121:501-539.
-
- Glover TJ. The bacteriology of cancer. Canada Lancet
Pract. 1930; 75:92-111.
-
- Haensch R, Seeliger H. Problems of differential diagnosis
of blastomyces and Russell bodies. Arch Dermatol Res. 1981;270(4):381-5.
-
- Hess D. Can Bacteria Cause Cancer? New York:New York
University Press; 1997.
-
- Jetha N, Priddy RW. Exact nature of Russell bodies still
an enigma. Am J Clin Pathol. 1984 Apr;81(4):545.
-
- King DF, Eisenberg D. Russell's fuchsine body. "The
characteristic organism of cancer". Am J Dermatopathol. 1981 Spring;3(1):55-8.
-
- Mattman LH. Cell Wall Deficient Forms (Ed 2). Boca Raton:CRC
Press; 1993.
-
- Mazet G. Corynebacterium, tubercle bacillus and cancer.
Growth. 1974; 38:
-
- McLaughlin RW, Vali H, Lau PC, Palfree RG, De Ciccio
A, Sirois M, Ahmad D, Villemur R, Desrosiers M, Chan E. Are there naturally
occurring pleomorphic bacteria in the blood of healthy humans? J Clin
Microbiol. 2002 Dec;40(12):4771-5.
-
- Nuzum JW. The experimental production of metastasizing
carcinoma of the breast of the dog and primary epithelioma in man by repeated
inoculation of a micrococcus isolated from human breast cancer. Surg
Gynecol Obstet. 1925; 11;343-352.
-
- Robinson DH.Pleomorphic mammalian tumor-derived bacteria
self- organize as multicellular mammalian eukaryotic-like organisms: morphogenetic
properties in vitro, possible origins, and possible roles in mammalian
'tumor ecologies'. Med Hypotheses. 2005;64(1): 177-85.
-
- Russell W. An address on a characteristic organism of
cancer. Br Med J. 1890; 2:1356-1360.
-
- Russell W. The parasite of cancer. Lancet. 1899;1:1138-1141.
-
- Scott MJ. The parasitic origin of carcinoma. Northwest
Med.
- 1925;24:162-166.
-
- Seibert FB, Feldmann FM, Davis RL, Richmond IS. Morphological,
biological, and immunological studies on isolates from tumors and leukemic
bloods. Ann N Y Acad Sci. 1970 Oct 30;174(2):690-728.
-
- Tedeschi GG, Bondi A, Paparelli M, Sprovieri G. Electron
microscopical evidence of the evolution of corynebacteria-like microorganisms
within human erythrocytes. Experientia. 1978 Apr 15;34(4):458-60.
-
- Wainwright M. Highly pleomorphic staphylococci as a cause
of cancer. Med Hypotheses. 2000 Jan;54(1):91-4.
-
- Wuerthele Caspe-Livingston V, Alexander-Jackson E, Anderson
JA, et al. Cultural properties and pathogenicity of certain microorganisms
obtained from various proliferative and neoplastic diseases. Amer J Med
Sci. 1950; 220;628-646.
-
- Wuerthele-Caspe Livingston V, Livingston AM. Demonstration
of Progenitor cryptocides in the blood of patients with collagen and
neoplastic diseases. Trans NY Acad Sci. 1972; 174 (2):636-654.
-
- Young J. Description of an organism obtained from carcinomatous
growths. Edinburgh Med J. 1921; 27:212-221.
-
-
- LEGEND FOR PHOTOGRAPHS (7)
-
- Figure 1. Tissue section of breast cancer showing (in
center) tightly-packed intracellular coccoid forms with some forms loosely
attached to the cell.
-
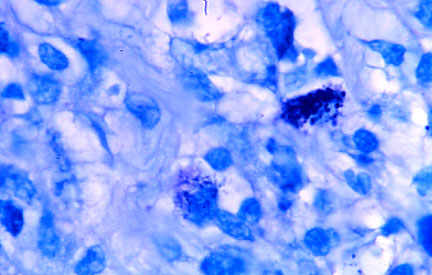
- Figure 2. Additional view of breast cancer showing two
areas (one below center and the other on the right) of intracellular
coccoid forms.
-
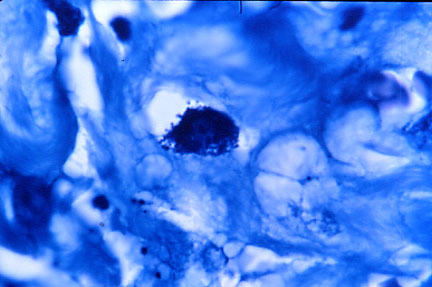
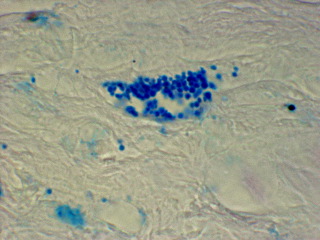
- Figure 3. Tissue section of lung cancer showing tightly-packed
intracellular coccoid forms.
-
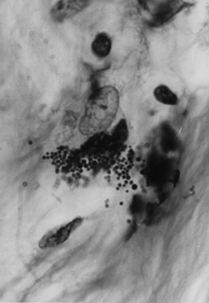
- Figure 4. Tissue section of Hodgkin's disease showing
intracellular and extracellular coccoid forms in the connective tissue
at autopsy.
-
- Figure 5. Tissue section of fatal AIDS-related Kaposi's
sarcoma of the skin showing two foci of coccoid forms.
-
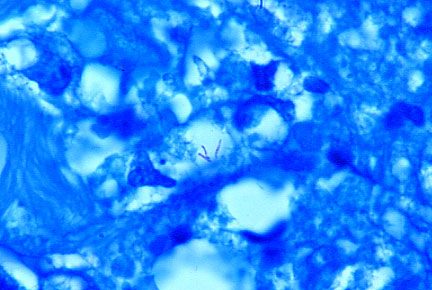
- Figure 6. Tissue section of fatal case of AIDS-related
immunoblastic sarcoma of the face. Three red-stained typical acid- fast
rods are seen in the center. These forms are extremely rare in cancer.
Mycobacterium avium-intracellulare was cultured from the tumor.
-
- Figure 7. Tissue section from prostate cancer showing
a focus of closely-knit coccoid forms as well as scattered forms.
-
-
- Alan Cantwell M.D.
- alancantwell@sbcglobal.net
- http://www.ariesrisingpress.com
- Author - AIDS & The Doctors of Death
- and Queer Blood
|