Hello Jeff - This is a list of just some parasites that the freeloading
savage invaders are bringing to Europe, the US and Canada and Australia
and New Zealand. The list of just some parasites is important because
it shows just a sample, a small one at that, of what German and Western
doctors are up against. No wonder the German health care system is ready
to break. Then there are all of the bacterial, viral and let us
not forget psychological diseases that the invaders have brought to the
west with them.
Diagnosing the various diseases that western doctors must identify is
very difficult. Often the doctors are dealing with migrants who
either cannot or will not speak the western language of the country they
are "invading." This compounds the difficulty in diagnosing. There
is also the fact that the Muslims and Black Africans get very violent
during examination. They refuse to allow women doctors and nurses
to examine them. The get extremely violent and have stabbed health
care professionals and some have had urine thrown in their face.
The Muslims and black Africans refuse to pay any of their doctor bills.
While spending so much time and resources treating and diagnosing the
Muslim and Black Africans there is little time and resources to treat
the citizens who actually PAY FOR THE HEALTH CARE SYSTEM.
If Hillary does get handed the election we need to familiarize ourselves
with this list of parasites as open borders will ensure that we, Americans
are going to see these parasites showing up in American citizens thanks
to Globalization.
When reading about the strain on the health care system in Europe and
Australia they should also mention the economic strain. Not one migrant
will ever pay their bills. Hillary wants to put all of these freeloaders
onto Medicare. How long do you think Medicare will be able to pay
for the invaders plus the American citizens who PAY FOR MEDICARE PREMIUMS
AND WHO PAY THEIR HOSPITAL BILLS?
Patty
Contents: Amebiasis; Giardiasis; Cryptosporidiosis; Malaria;
Visceral leishmaniosis; Toxoplasmosis; Schistosomiasis; Clonorchiasis;
Fascioliasis; Echinicoccosis; Toxocariasis; Capillariasis; Pentostomiasis).
Amebiasis
Among various amebas, the Entamoeba histolytica is the one that invades
tissues in man. As long as it remains in the lumen of the colon (luminal
phase), it causes no problems. When it invades the bowel wall (invasive
phase) it causes a diarrhoic syndrome and may spread to the liver where
it forms amebic abscesses which are usually solitary. The patient experiences
pain and tenderness in that region and general symptoms with fever. The
diagnosis of abscess is made with imaging techniques. The diagnosis of
amebiasis is made by serological tests for amebic antibodies. The treatment
is by drugs and rarely surgical. The first association of ameba with liver
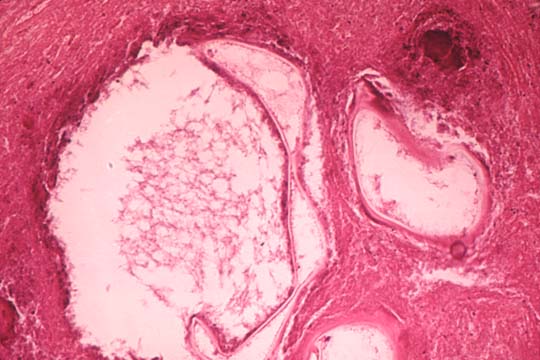
abscess was described by Loesch in St. Petersburg, Russia, in 1875.The
figure shows clusters of ameba trophozoites in the tissue, large, up to
60 microns in diameter. This is the active mobile form. They have one
small eccentric nucleus and cytoplasmic vacuoles sometimes containing
red cells. The cystic form with round shape and multiple nuclei does not
occur in the tissues.
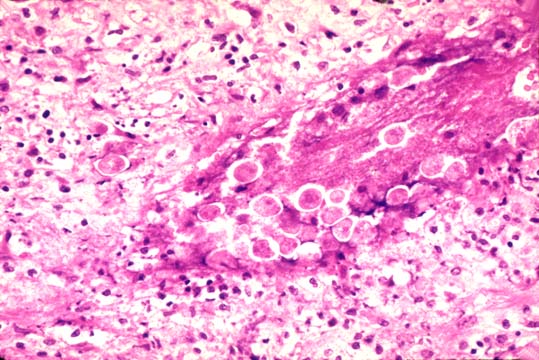
Entamoeba histolytica
Clusters of trophozoites in the tissue, large, up to 60 microns in diameter.
This is the active mobile form. They have one small eccentric nucleus
and cytoplasmic vacuoles often containing red cell. The cystic form with
spherical shape and multiple nuclei does not occur in the tissues.
Giardiasis
This organism causes a diarrhoic syndrome. It rarely affects the liver
where it can cause cholecystitis, cholangitis and granulomatous hepatitis.
The diagnosis is made with light microscopy in the stools. This flagellate
protozoan represents a historical curiosity. It was first seen by the
inventor of the microscope, Leeuwenhoek, in 1881, in his own stools. Its
pathological significance, however, was recognized tow hundred years later
by Lambl of Prague in 1859. The organism in its tropho stage is flat,
rounded at one end and pointed at the other end. It has tow paired nuclei
and 4 pairs of flagella. The encysted form is smaller without flagella
and four nuclei.
Cryptosporidiosis
Cryptosporidium is a parasite of domestic and wild animals. In normal
humans it causes no damage but in immunocompromised individuals it can
cause a protracted diarrhoic syndrome and cholecystitis and cholangitis
in the liver. The diagnosis is made by light microscopy. This organism
is acid-fast positive.
Malaria
There are four species of Plasmodium that cause disease in humans: P.
falciparum, P.malariae, P. vivax, P. ovale. They have a sexual life cycle
in the mosquito (sporogony) and an asexuals cycle in humans (schizogeny)They
are transmitted by the female of the Anpheles mosquito. With their bites
they inject sporozoites of these plasmodia into the blood stream. The
organisms concentrate and proliferate in the liver where they form paranuclear
masses( schizontes) visible even with a light microscope. Individual organisms
(merozoites) are released from these masses and go to infect and destroy
red cells. Schizontes of P.vivax and ovale may stay in hepatocyte for
long time (hypnozoites) and cause relapses at distance of months and years;
schizontes of P.falciparum and malariae do not have a long hepatic phase
and develop into schizontes and merozoites in the red cells, capable to
reinfect red cells but not hepatocytes. Gametocytes which develop from
merozoites are sucked by mosquitoes to infect other individuals. There
are, in summary two phases: extraerythrocytic and erythrocytic. Infected
red cells will stick to endothelial cells of capillaries causing sequestration
of red cells and disfunction of the microcirculation (anoxia) in various
organs and fever. P.vivax and ovale cause benign tertian malaria; P. falciparum
causes malignant tertian malaria; P. malariae causes quartan malaria.
The malarial attacks consist of chills and fever recurring at 48 hour
intervals for tertian and at 72 hour intervals for quartan type. Each
attack lasts for-12 hours and coincide with the rupture of erythrocytes
and release of a new pousse' of organisms. Hepatic involvement is rare
and consists of Kupffer cell hyperplasia, deposition of malarial pigment,
coarse, dark-brown(hemozoin), derived from hemoglobin altered by the plasmodium,
in Kupffer cells and portal macrophages. It is negative for stainable
iron. The hepatocytes show some non-specific unrest. Severe jaundice and
cetrilobular necrosis similar to viral hepatitis may occur with falciparum
infection. In tropical splenomegaly syndrome consisting of splenomegaly,
thrombocytopenia and lymphocytosis, the liver may show marked sinusoidal
lymphocytosis similar to infectious mononucleosis.
Visceral leishmaniasis (kala-azar)
It is due to Leishmania donovani transmitted by sandflies, Phlebotomus
in Eurasia and Africa and by Lutzomya in Brasil. It is endemic in the
Mediterranean basin India, Northern China, east Africa and Brazil. Dogs
and rats appear to function as reservoirs. The clinical picture consists
of fevers , malaise and progressive hepatosplenomegaly lymphadenopathy,
pancytopenia, cachexia. The spleen becomes lather hard. The liver contains
numerous L-D bodies in Kupffer cells stainable with H&E and Giemsa.
There is effective treatment with pentavalent antimonials, aromatic diamadines
and amphotericin B.
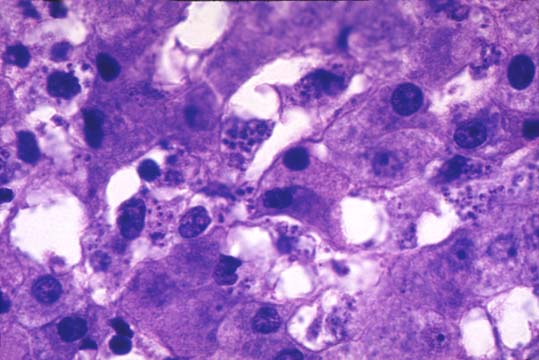
Leishmania donovani
Clusters of rounded bodies, 2-3 microns in length inside macrophages and
endothelial cells in hepatic sinusoids. This is the leishmania form. In
culture and in insects they exist as flagellated form with a single long
flagellum.
Toxoplasmosis
It is due to Toxoplasma gondii, so-called because it was found in a rat
by the name gondi in North Africa. It is acquired from raw meat and cat
feces. It affects immunosuppressed individuals. It is a major intercurrent
infection in cardiac and liver transplants. Fetuses are infected from
the placenta and develop severe brain damage. Fluorescent antibody test
for IgG and IgM are the best for diagnosis. It is readily seen in H&E
sections. It is treatable.
Schistosomiasis
Schistosoma are trematodes (flat worms). The species that cause infestation
in men are: S. mansoni, S. japonicum , S. intercalatum, S. mekongi which
parasitize the intestinal venules and capable of spreading to the liver
and Schistosoma hematobium which resides in the vesical venules and damage
the urinary bladder and ureters. The first of these parasites (hematobium)
was discovered in Egypt in 1852 by a German pathologist, Bilharz. These
organisms infect millions (200) of people in Asia , Africa and South America
mainly Egypt, Nigeria, China (japonicum), Subsaharan Countries and Caribbean
islands, Brazil and Venezuela in the Americas(mansoni).S.hematobium Is
scattered trough Africa bu it is concentrated in the Nile valley. Man
contracts the infection from fresh water snail which release the cercarial
form of the worm in the water. The cercariae are motile and penetrate
the human skin or mucosae, enter the circulation, pass through the lungs
ad lodge in the hepatic branches of the portal vein where they become
adult worms, male and female. They copulate, leave the liver and migrate
to the fine intestinal radicals of the inferior mesenteric vein especially
around the colon and rectum. The S. mansoni and japonicum reach the little
venules of the colonic and rectal submucosa where the female releases
her ova. The eggs erode the mucosa and fall into the colonic lumen, are
defecated and go to infect other snails where new cercariae are formed
thus restarting the cycle. Many ova from the colonic mucosa instead of
being extruded into the intestinal lumen are extruded into the portal
circulation, they reach the liver where they produce the typical periportal
fibrosis. Sometimes in the case of S.mansoni, adult worms are seen in
the hepatic branches of the portal vein. The mature worms are flat and
measure 10 to 16 mm in length depending on the species. The female is
thinner and longer than the male. The ova vary in size and shape according
to the species. The ova of S.mansoni have a characteristic lateral spine.
The morphological changes in the liver consist of granulomas with giant
cell, epithelioid cells containing ova of the parasite. The granulomas
are mostly located in the portal fields where they produce a stellate
fibrosis of "clay pipestem"type which is appreciated in the cut surface
of the liver. This fibrosis produces portal hypertension due to occlusion
of portal vein radicals but does not cause cirrhosis. If there is cirrhosis
it is due to hepatitis B associated with schistosomiasis in the same geographic
areas.
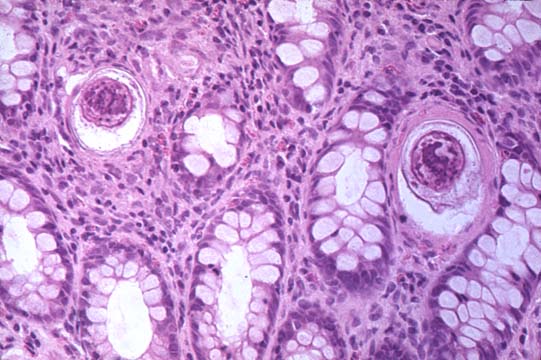
Schistosoma mansoni
Eggs in the venules of the intestinal mucosa which are shed into the intestinal
lumen and the environment where they release their miracidia which go
to parasitize the snails. The eggs are about 150 microns in maximum diameter.
The lateral spine cannot be seen in this section.
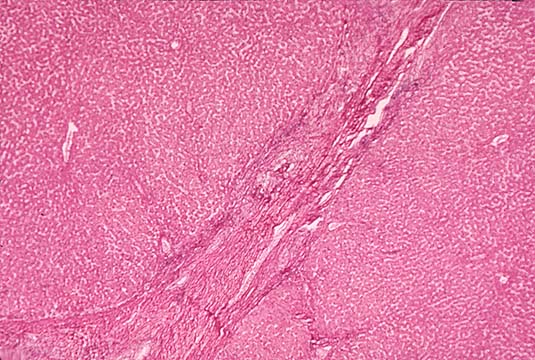
Schistosoma mansoni
Section of infested liver with periportal fibrosis which, on cut section
is so dense as to resemble a pipe stem.
Clonorchiasis
Clonorchis (opistorchis) sinensis is a flat fluke, 10-25 mm in length
and 3-5 mm in width, reddish, transparent that resides in the major intrahepatic
bile ducts. It is found mainly in the Far East. It is acquired by eating
row or poorly cooked fish which carry the eggs of this parasite in their
scales. The infection causes dilatation of intrahepatic bile ducts resembling
cysts and may cause purulent cholangitis with multiple liver abscesses
due to E.coli. The presence of the fluke induces glandular hyperplasia
of the bile ducts with increased mucus secretion. The glandular hyperplasia
may be prominent and adenomatous. Cholangicarcinoma is associated with
this infestation. Other tow similar trematodes are found in Poland and
Siberia (Opistorchis felineus) and in Thailand (Opistorchis viverrini).
They cause a disease similar to O.snensis and are associated with cholangiocarcinoma.
Fascioliasis
Fasciola hepatica (sheep liver fluke) is a fluke measuring about 30mm
in length and 13mm in width. The distribution is world-wide especially
in sheep-raising countries. It is acquired by ingestion the cercariae
which develop in the snails and are released in the grass near water streams.
After being ingested with grass by sheep or by humans with watercress
salad, they penetrate the duodenal wall and enter the peritoneum. They
penetrate into the liver through the glissonian capsule and lodge in the
bile ducts producing obstruction but not cholangicarcinoma. The liver
may show indurated nodules at the surface which indicate the passage of
the parasite. Hepatitic colic , jaundice and fever may be part of the
symptoms in humans. It may cause bleeding and anemia. In the middle East
this parasite may cause a syndrome named halzoun which is a suffocating
illness due to lodging of the parasite in the pharynx due to ingestion
of contaminated sheep livers. It is treated with emetine hydrochloride.
Echinococcosis (Hydatid Cyst)
It is due to the larval form of short tapeworms of the genus Echinococcus.
The species of Echinococcus granulosus is the most common. The cystic
disease was known to Hippocrates but it took about 2000 years to identify
the responsible agent, the worm, which was discovered only in 1808 by
Rudolphi in Germany. The worm is 3 to 6 mm long and lives attached to
the villi of the small intestine of canines (dogs and foxes).It has a
head and three proglottides the terminal being the one gravida with eggs.
It lives between 5 and 20 months in the dog and when it is evacuated,
the gravid proglottis bursts releasing the eggs. The eggs are picked up
and ingested by the intermediate hosts that can be sheep, hogs ,ox and
man . In the can expand to a large size. Their wall is made of a thick
cuticle with an inner layer of proliferation of the parasite, protoscolices,
small cysts containing scolices which, like granules fall in the lumen
full of liquid and may form daughter cysts. The scolices contain suckers
and hooklets which can be seen under the microscope. Rupture of the cyst
will disseminate the infection and may result in a serious anaphylactic
shock. Dogs that eat the cysts will develop the terminal form of the worm
in their intestine. Diagnosis is made by serology. Treatment consists
of surgical removal of the intact cyst. A more aggressive variant of echinococcosis
is produced by Echinococcus multilocularis. The terminal host is the fox
and the intermediate hosts are rodents. The cysts are multiple and smaller.
Humans can contract it. It is found around the Alps, Alaska, Canada, China.
It is More aggressive and more difficult to control than Echinococcus
granulosus.

Echinococcus granulosus
Liver with a hydatid cyst containing fluid and daughter cysts. Notice
the thick connective tissue capsule which cannot be broken in attempting
to remove the cyst.
Histological section of
the above
Section of daughter cysts showing the germinal layer with attached scolices.
Ascariasis
It is due Ascaris lumbricoides, the giant round intestinal worm. It has
world wide distribution. It is acquired by ingesting the eggs which are
produced by the female in millions. In the duodenum, the larvae of these
eggs penetrate the wall, enter the mesenteric lymphatics or the hepatic
venules and reach the heart and the lungs. Here they invade the air spaces
and through bronchioli and bronchi they reach the epiglottis and are swallowed
in the stomach able to resist the gastric juices. They reach the intestine
and mature into males and females an restart the cycle. From the lungs
they may reach the left heart and become distributed to every organ where
they cause acute tissue reactions. The larvae in the lungs may cause ascaris
pneumonitis: Mottling of the lungs, dyspnea, high fever. In the liver
, the larvae may produce granulomas. The adult worms in the intestine
cause colicky pains and fever in children, also, appendicitis, blockage
of the ampulla of Vater and common bile duct, hemorrhagic pancreatitis.
Metabolites of the worm cause sensitization phenomena: bronchial asthma,
urticaria, conjunctivitis , palpebral edema. There is efficient treatment
with hexylresorcinol.
Toxocariasis.
Toxocara canis and T.catis are intestinal ascarids of dogs and cats. In
humans, their ingested larvae migrate to the liver where they form granulomas
in the portal tracts. The disease is more frequent in children being more
in contact with dogs. The liver is the most affected organ. Here the granulomas
can be seen as small-size whitish spots under the capsule. Invasion of
other organs may also occur. The granulomas are mostly composed of eosinophil
with some histiocytes at their periphery. There may be rare giant cells.
The larva in these granulomas is not always seen, but their morphology
with the history of exposure to dogs is sufficient for the diagnosis.
There are no reliable serological tests. The prognosis is favorable in
the majority of cases. The infection of the eye requires enucleation.
Administration of antielmintics to dogs and cats is the best method of
prevention. There is no specific therapy.
Capillariasis
It is due infestation with Capillaria hepatica, a common worm parasite
of rats, and les commonly of squirrels, maskrat, hare beaver, chimpanzee
and other monkeys. Few cases have been reported in man. The worm liver
in the liver where it deposits its eggs. The eggs cause necrosis and fibrosis
in the li and are not released in the feces.The infestation is contracted
by injesting the infected liver. The worm and and eggs resemble Trichuris.
The eggs have a birefringent. There is no treatment.
Pentostomiasis
Is due to "tongue worms", because the adult forms are elongated like tongues.
Two genera affect man, Armillifer armillatus and Linguatula serrata. They
live mainly in the respiratory passages of snakes but also in birds and
nares of mammals where they produce eggs which are released in the environment.
Contamination occurs by ingesting the eggs with larvae which spread through
various organs forming encysted ninphae which at the surface of the liver
form small encapsulated whitish nodules very similar to fasciola infestation.
http://www.lumen.luc.edu/lumen/meded/orfpath/parinf.htm |
